
Practitioner Seed #4 : Understand Load & its Effects!
Arnold Schwarzenegger understood load & how to prescribe it to himself!
He knew precisely how many Kilograms to bench press, how many sets & reps to push, tempo, work: rest, How frequent to train, how much recovery to take………..
His objective: build the man mountain Juggernaut!
Ok maybe there were some synthetic enhancements involved!
The point being, when we prescribe exercise, it is critical we understand the effect that a load has on the patient in front of us.
Arnie squatting 250kg might be equivalent to an elderly osteopenic woman completing 5 sit to stands.
To further understand load we take a trip back to our high school physics class………..
Load = Physical forces applied to tissues
The effects of these physical forces results in deformation of tissue, a cellular response, inter -cellular signalling and finally a structural change to the tissue.
Mechanotherapy, Mechano-transduction, Mechano-biology
Terms that have gained momentum in the scientific literature and provide a solid explanation for the things we have been doing for years as a sports rehab practitioner.
A seminal paper by Karim Khan & Anthony Scott – B2W-43-04-0247.pdf (nih.gov) – A must read if you haven”t already!
Its important to remember that load does not exclusively affect structure at the tissue level. Neurology and psychology play important roles in response to load. Check out Erik Meira’s (The Science PT ) eloquent analysis of how load affects multiple systems, not only structure – https://thesciencept.com/just-load-it/
When we are thinking at the tissue level, developing an appreciation for how certain tissue types respond under certain loading conditions, is paramount to creating an effective exercise program.
Whilst we have scientific evidence combined with expert opinion, that combined compressive + tensile forces can be detrimental to tendon health (mid substance or entheses), if we take these same forces and apply to a different tissue, say mid shaft of bone, there is no adverse effect.
The bone cells are not perturbed in the slightest!
An athlete produces a 600kg/f Quadricep contraction, the patella tendon experiences this as tensile force and is delighted to receive such a gift!
Then we see the marathon runner who increases their training load by 25% over a week while they might already exhibit midfoot hyper pronation. The distal medial tibia experiences a spike in tensile (distraction) forces, suffers some bone marrow oedema and the athlete begins to develop shin soreness.
When we think about loading tissues it’s a lesson in Horses for Courses!
One feature of load that is common among all tissue injury responses is:
Rate of Loading
Muscle strains occur during ballistic eccentric contractions.
Tendinopathy occurs after a spike in high elastic/ energy storage loads.
ACL’s rare reported to rupture in potentially the first 0-61ms after initial contact (4).
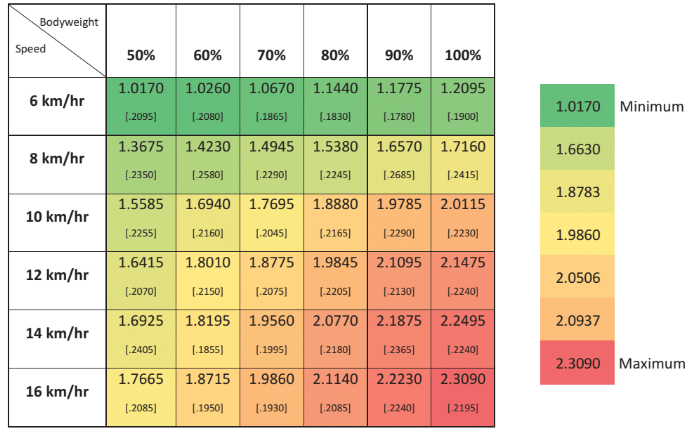
Here we have some nice work from the guys at Aspetar highlighting that running speed (aka rate) has more affect over total plantar force (multiples of BW) than increases in % total body weight, as measure on an anti -gravity treadmill (AlterG). (Thomson et al, 2017). A nice indication that rate of loading is more pertinent to the total load going through the foot, than overall magnitude of force.
‘Begin with the end in mind” – Habit 2 Stephen Covey’s “7 Habits of a Highly Effective Person
This applies to our rehabilitation planning.
We must first understand how much force this injured tissue will need to withstand, and how quickly it will need to dissipate these forces.
Tissues might faces 3 multiples of body weight during walking, 6-8 during running and upwards of 12 during sprint, jump & land & accel/ decels.
So we need to prepare our injured tissue to a satisfactory level!
Where does 3 sets of 10 come from?
Our subconscious default throughout our student days is to prescribe 3×10.
While 3×10 might buy some adaptation in some of the lower trained populations, take this to the athletic arena, and you will be left with egg on your face!
This is where we need to think critically.
What are we chasing:
- Pure Force production
- Hypertrophy
- Fatiguability
- Kinetic chain coordination
- Rate of force development (Strength-Speed, Speed-strength & plyometric)
- Rate of force acceptance – A big one in the injury domain!
- Joint angle specific
- Contraction mode specific
- Collagen adaptation
- Analgesia
When your patient or athlete presents with a past history the size of Arnolds Quadricep, there is no doubt that levels of fear and anxiety have created the perfect environment for descending inhibition to do its thing, if they haven’t already become fear avoidant.
Combine this with hearing of their team mate suffering a similar injury that ended their career, and the stress that surrounds putting pen on that upcoming contract renewal, you now have a bigger beast to deal with than purely that wretched L5 Annular tear.
This is where you need to think about load from a different perspective. Consider:
- Pain education
- Pacing strategies
- Counselling regarding past experiences
- Graded exposure
- Language
- Societal effects
All as elements of load.
Congratulations, you now understand the basic premise of load in the context of the
Bio: Weights, speeds, reps, sets etc, affecting tissues.
Psycho: Beliefs, fears, attitudes.
Social: Norms, attitudes, narratives
Approach!
For a more in depth analysis of load, exercise prescription and rehab planning head on over and sign up to Principles of Exercise Prescription – Clinicalx foundations
Reference
2.
(2017) Running speed increases plantar load more than per cent body weight on an AlterG® treadmill, Journal of Sports Sciences, 35:3, 277-282,
4. Bates, N. A., Schilaty, N. D., Ueno, R., & Hewett, T. E. (2020). Timing of Strain Response of the ACL and MCL Relative to Impulse Delivery During Simulated Landings Leading up to ACL Failure, Journal of Applied Biomechanics, 36(3), 148-155. Retrieved Feb 7, 2022, from https://journals.humankinetics.com/view/journals/jab/36/3/article-p148.xml
Comments (0)